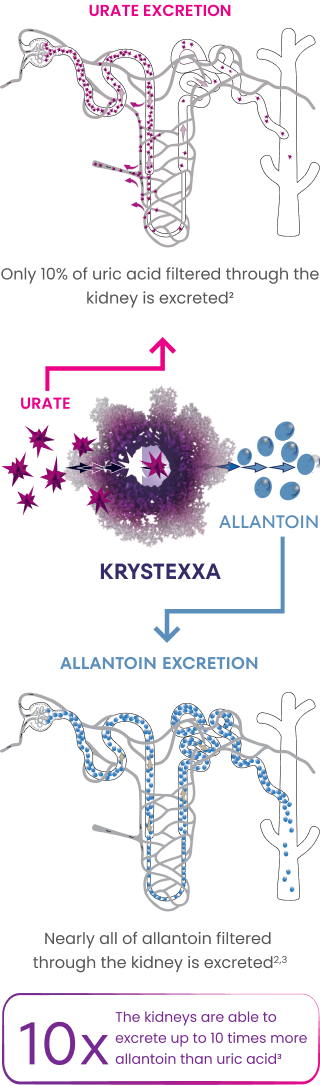
KRYSTEXXA is an infused biologic that converts urate into allantoin2





The KRYSTEXXA team is available to share more about the benefits of reducing ADAs.
See how KRYSTEXXA and methotrexate reduces sUA and resolves tophi quickly.

Occupation:
Accountant
55-year-old with hypertension diagnosed with gout 4 years ago
Actor portrayal, not actual patient.

Occupation:
Middle school teacher
52-year-old with diabetes diagnosed with gout 15 years ago
Actor portrayal, not actual patient.

Occupation:
Stay-at-home parent
43-year-old diagnosed with gout over 20 years ago
Real patient.
KRYSTEXXA is not indicated for the treatment of pain.
Gout Flares: An increase in gout flares is frequently observed upon initiation of anti-hyperuricemic therapy, including KRYSTEXXA. Gout flare prophylaxis with a non-steroidal anti-inflammatory drug (NSAID) or colchicine is recommended starting at least 1 week before initiation of KRYSTEXXA therapy and lasting at least 6 months, unless medically contraindicated or not tolerated.
Congestive Heart Failure: KRYSTEXXA has not been formally studied in patients with congestive heart failure, but some patients in the pre-marketing placebo-controlled clinical trials experienced exacerbation. Exercise caution in patients who have congestive heart failure and monitor patients closely following infusion.
The most commonly reported adverse reactions (≥5%) are:
KRYSTEXXA co-administration with methotrexate trial:
KRYSTEXXA with methotrexate: gout flares, arthralgia, COVID-19, nausea, and fatigue; KRYSTEXXA alone: gout flares, arthralgia, COVID-19, nausea, fatigue, infusion reaction, pain in extremity, hypertension, and vomiting.
KRYSTEXXA pre-marketing placebo-controlled trials:
gout flares, infusion reactions, nausea, contusion or ecchymosis, nasopharyngitis, constipation, chest pain, anaphylaxis, and vomiting.
KRYSTEXXA® (pegloticase) is indicated for the treatment of chronic gout in adult patients who have failed to normalize serum uric acid and whose signs and symptoms are inadequately controlled with xanthine oxidase inhibitors at the maximum medically appropriate dose or for whom these drugs are contraindicated.
Limitations of Use: KRYSTEXXA is not recommended for the treatment of asymptomatic hyperuricemia.
Please see Full Prescribing Information, including Boxed Warning.